

INTRODUCTION
Spontaneous intracerebral hemorrhage (ICH) accounts for 10-20% of all strokes (4 million patients worldwide each year) and is the deadliest subtype of stroke with up to 40% of median mortality at 1 month, 50% at 1 year [1-3]. Among survivors, 61-88% are dependent on others for activities of daily living 6 months after the hemorrhage [3]. Considering the high mortality and morbidity, there is no doubt that a huge and life-threatening ICH (Glasgow Coma Scale≤8, and volume≥30 cm3) should evaluated and investigated for therapeutic strategies [4].
Although craniotomy or decompressive hemicraniectomy has been postulated as a feasible and relatively well-tolerated treatment option for selected patients [5], any kinds of surgery to reduce the volume of ICH have clinical and experimental evidence because ICH mass removal might reduce increased intracranial pressure (IICP), nervous tissue damage by relieving local ischemia or removal of noxious chemicals [6-11]. Thus, surgical options have been repeatedly evaluated in large multi-center randomized controlled trials (RCTs). One of the most representative RCTs, the International Surgical Trial in Intracerebral Hemorrhage (STICH), has concluded that patients with spontaneous supratentorial ICH in neurosurgical unit show no overall benefit from early surgery when compared with initial conservative treatment [12]. STICH II trial confirmed that early surgery does not increase the rate of death or disability at 6 months and might have a small but relevant survival advantage for patients with spontaneous superficial ICH without intraventricular hemorrhage (IVH) [13]. Besides STICH trials, there are many reported RCTs including the National Institutes of Health sponsored Minimally Invasive Surgery Plus recombinant tissue plasminogen activator (rt-PA) for ICH evacuation (MISTIE) trial evaluating stereotactic thrombolysis, the endoscopic arm of MISTIE referred to as the Intraoperative Stereotactic Computed Tomography-Guided Endoscopic Surgery trial, the Early Minimally-Invasive Removal of Intracerebral Hemorrhage trial and the Minimally Invasive Endoscopic Surgical Treatment With Apollo/Artemis in Patients With Brain Hemorrhage [14]. Although most recently reported MISTIE III trial concluded that MISTIE did not improve the proportion of patients who achieved a good response 365 days after ICH [15], many other studies including meta-analysis reported that the minimally invasive procedures especially for endoscopic evacuation, seem to be more effective than conservative treatment in reducing both morbidity and mortality [16-20].
Stereotactic thrombolysis and ICH aspiration is the most widely studied minimally invasive surgical technique. Although many prior reports reported limited benefit after stereotactic aspiration, recent advances using thrombolytic agents have allowed for greater hematoma aspiration without an increase in clinically symptomatic procedure-related bleeding.
Therefore, the purpose of this article is to demonstrate the minimally invasive ICH aspiration procedure using Cosman-Roberts-Wells (CRW) stereotactic frame.
Cosman-Roberts-Wells stereotactic frame and surgical technique
Theodore Roberts and Russel Brown first developed the Brown-Roberts-Wells system (BRW) at the University of Utah, collaborating with biomedical engineering developer Trent Wells [21]. This system included location of a three-dimensional (X, Y, Z) coordinate in space by utilizing two dimensions (X, Y) defined by imaging studies, such as computed tomography (CT) or magnetic resonance imaging (MRI) and adding a vertical coordinate (Z). Any three-dimensionally defined points in space could be reached directly. The BRW guidance system consists of five functional components: a head ring, a localizing system, an arc guidance system, a phantom simulator, and a floor stand [21]. The ring is attached to the patient’s cranium with screws that are tightened into the skull [21]. The localizing system, consists of six vertical and three diagonal graphite rods, is secured to the head ring with three ball-and-socket interlocks, creating an N-shaped appearance [21]. This N construct establishes the axial CT scan section relative to the skull base by calculating the relative distance of the oblique to the vertical rods [21]. Target coordinates are established by identifying the axial slice that best shows the desired target [21]. The BRW system then further includes a movable arc and a probe holder. The arc guidance frame has four motions that create infinite different probe pathways [21].
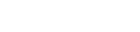
The CRW stereotactic frame is an arc-radius system developed to utilize the aforementioned components of the BRW system to localize target coordinates. The CRW system consists of five major components: the standard BRW base ring, an MRI or CT localizer unit, an arc-radius frame, a phantom simulator (Fig. 1). The target localization is performed according to the base ring fixed to the skull at four pin sites, and image-directed target coordinates with the MRI or CT localizer unit affixed to the base ring by way of three ball-in-socket joints. Target coordinates are then input into the phantom simulator and CRW frame to assure correlation. The system is then utilized to stereotactic procedures, such as targeting catheter placement or deep brain stimulation electrode placement. Benefits to the arc-radius design include the capability of infinite non-predetermined entry points. With the use of specially designed partial arcs, lateral placement of the base ring is also possible.
Calculating target coordinates from axial computed tomography scans
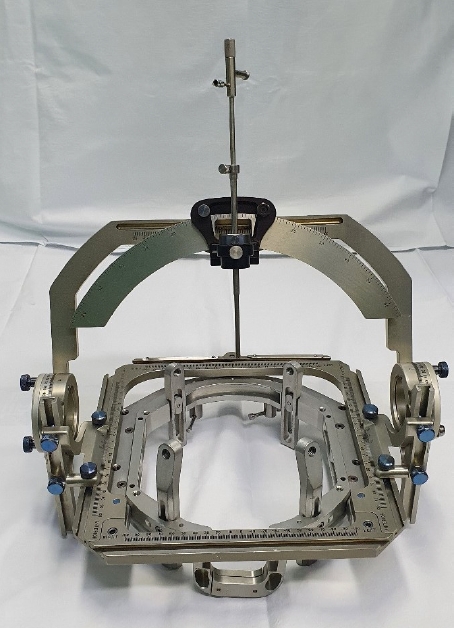
The operator select a best axial slice that shows the desired target. Then, locate rod 1 on the patient’s right posterior and rod 7 on the patient’s left anterior. Draw a line connecting the centers of those two rods. After connecting the two rods, locate rod 3 on the patient’s right anterior, and rod 9 on the patient’s left posterior. Draw a line connecting the centers of those two rods. The intersection of these two lines coordinates the central point (0, 0) of X, Y axis (Fig. 2A). After confirming the central point, measure the anterior-posterior and lateral distances from the central point (0, 0) to the desired target (Fig. 2B). The vertical coordinate (Z) can be calculated by measuring the distance from the center of rod 1 to the center of rod 2, recorded as Z1. The center to center distance between rods 7 and rod 8 can be recorded as Z2. The value Z is defined as [Z1+Z2]/2 and the vertical coordinate is defined as Z-60 mm (Fig. 2B).
All operations are performed under general endotracheal anesthesia. The axial 0.5 cm thickness CT slices are obtained spanning the ICH. Generally, the ipsilateral frontal standard burr hole location (3 cm lateral to midline and just anterior to the coronal suture) is typically used for basal ganglia and thalamic hemorrhages. If the ICH is lobar in location or extended to the cortical surface, the burr hole is localized over the ICH. A silicone catheter with small openings at its proximal ending over a length of 1.5 cm, is placed with the introducer cannula into the ICH via frame-guided pre-calculated coordinates to perforate the center of the ICH. Any instruments to disrupt the ICH mechanically, do not used. Then, the rigid introducer cannula is removed carefully. After removing the introducer catheter, careful manual ICH aspiration is attempted using a syringe. After placement of ICH catheter within the center of hematoma, the catheter is tunneled subcutaneously away from the burr hole and skin incision is closed. The ICH catheter is connected to a three-way stopcock to allow for injection of thrombolytics such as urokinase or rt-PA and saline in addition to drain ICH. Immediately after the operation, the CT scan is repeated for assessment of catheter placement and residual ICH volume. Catheter replacement is performed if necessary.
In selected patients, urokinase or rt-PA are administered through the catheter. Generally, the volume of administered urokinase is 5,000 IU/1 mL saline or 3,000 IU/2 mL saline and subsequently flushed with 1-2 mL of saline and then clamp. After 30 minutes, the catheter is released and natural drainage of liquefied ICH is maintained. This procedure is repeated at 8-hour intervals until the ICH volume decreased to <25 mL, less than half of the preoperative volume, 10 urokinase instillations or 72 hours after the operation [22,23]. Injection of rt-PA starts six hours after a postoperative CT scan confirms periprocedural clot stability. Then, rt-PA is injected every 8 hours and up to 9 injections. Injection of rt-TA is stopped when the ICH volume was decreased to <15 mL. CT scans is performed daily to measure remaining ICH volume and evaluated ICH stability. The ICH catheter is allowed to drain for 24 hours after sufficient reduction of the ICH or 25 hours after the last dose of rt-PA before it is removed [24].
The patient was maintained on prophylactic intravenous antibiotics until the ICH catheter was removed. The catheter was removed at the bedside under sterile technique.
CASE REPORT
Case 1
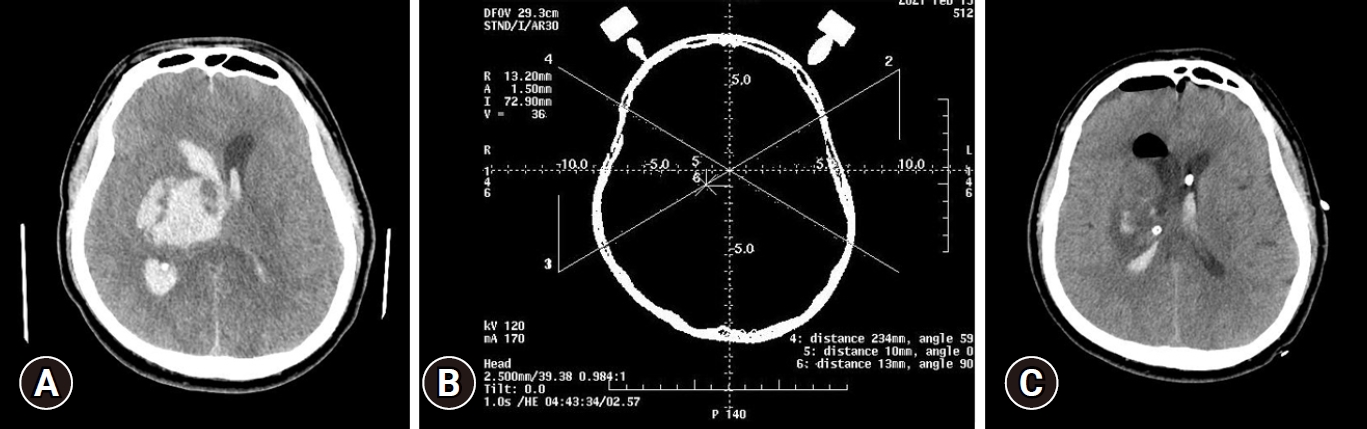
A 59-year-old male with hypertension was admitted to the emergency department with suffering for mental change and left hemiparesis. Preoperative CT showed acute ICH in right basal ganglia, thalamus, and IVH (Fig. 3A). The CRW stereotactic frame was fixed on four sites of patient’s head with head ring screws. And then, CT scan to acquire the coordinates was checked (Fig. 3B). The patient was transferred to operation room and the patient’s head was fixed on operating table after general anesthesia. The coordinates were set on arc system and the arc system was attached to CRW frame on patient’s head. External ventricular drainage catheter was inserted in left lateral ventricle and drainage catheter was clamped immediately due to prevent brain shifting. After that, trephination hole was made for hematoma aspiration in right frontal area. ICH was aspirated using aspiration cannula and 12F drainage catheter was placed hematoma site. Drainage catheter placed ICH site was removed after CT scan three days after operation (Fig. 3C).
Case 2
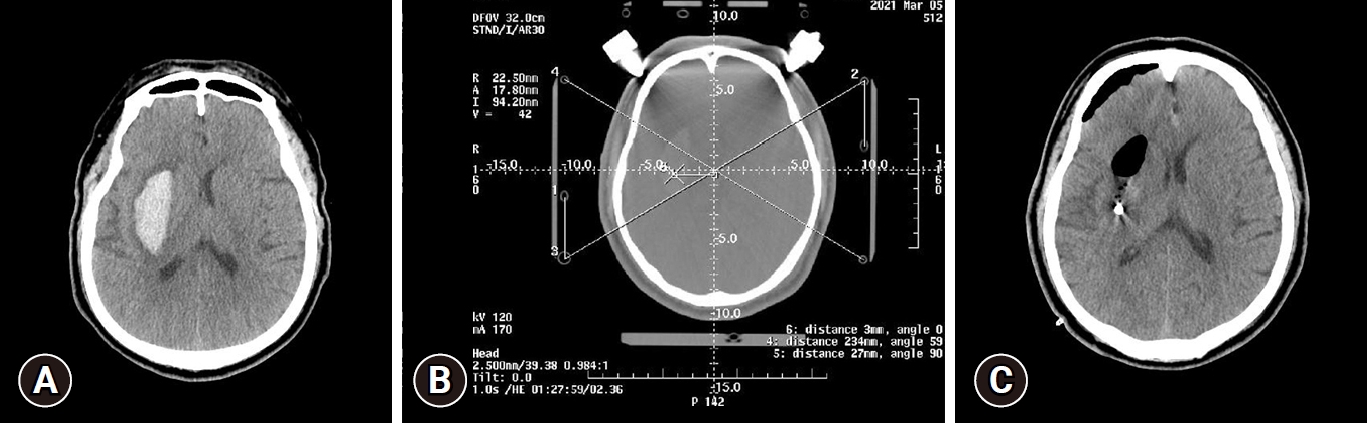
A 65-year-old male without any significant previous medical history was admitted to the emergency department with left hemiparesis. Preoperative CT showed acute ICH in right basal ganglia (Fig. 4A). The CRW stereotactic frame was fixed on patient’s head under local anesthesia infiltration. After CT scan for stereotactic surgery (Fig. 4B), the coordinates were calculated. The patient’s head was fixed on operating table with Mayfield adapter and arc system set for coordinates was attached CRW frame. Trephination hole was made in right frontal area using drill, ICH was aspirated using aspiration cannula and drainage catheter was placed hematoma site. Drainage catheter was removed after CT scan three days after operation (Fig. 4C).
DISCUSSION
The treatment of patients with ICH remains controversial. Historically, craniotomy had been hypothesized as an appropriate treatment for ICH evacuation. However, STICH trial revealed that there was no overall benefit from early surgical intervention for spontaneous supratentorial ICH as compared with initial conservative management [12,13]. Many surgical trials confirmed that the benefits from craniotomy are marginal at best and moreover, craniotomy would be more harmful than beneficial because of tissue damage without improved clinical outcomes [25].
Although many previous study reported the non-superiority of surgical intervention, the current conservative treatment would be insufficient, especially in patient with severe space-occupying hemorrhage and secondary deterioration. For these patients, conventional decompressive craniectomy may be beneficial to lower ICP, improve cerebral perfusion, and relieve peri-hematomal edema [26]. The principal goal of surgical intervention is reducing hemorrhage volume, preventing further hemorrhage, relieving mass effect, and reducing ICP rapidly, thereby preventing secondary neurological deterioration by relieving local ischemia or removal of noxious chemicals. The STICH II results also showed that patients with hematomas at a distance of 1 cm from the cortical surface were more likely to have favorable outcome from early surgery than those with deep hematomas [13].
Several efforts have been performed to minimize the invasiveness of surgical procedures. In recent years, the utilization of minimally invasive surgery including stereotactic aspiration or endoscopic evacuation to remove ICH is recognized as more helpful than conventional craniotomy in reducing postoperative complications and in increasing survival rates [16]. Although most recent reported multicenter RCT, MISTIE III, demonstrated that aspiration and thrombolytic irrigation of ICH with rt-PA did not improve functional outcomes compared with standard medical care group, the mortality rate at 7 days, at 30 days and at 365 days seemed to be lower in the MISTIE group than standard medical care group [15]. They also reported that for those patients who achieved hematoma volume reduction to below 15 mL, there was a significant improvement in modified Rankin Score at 365 days [15]. Nevertheless, the results of the MISTIE trials support the need to evaluate ICH evacuation technique more thoroughly.
Frame-based stereotactic surgical technique is a well-established procedure providing the neurosurgeon with the ability to accurately approach almost any region of the intracranial area, and the capability to place intracranial catheter to drain any kinds of fluid to reduce IICP. This technique has been regarded as a safe procedure compared with other conventional surgical technique such as craniotomy because of less procedure-related morbidity and mortality rate. Numerous frame-based stereotactic systems are currently used in clinical practice to evacuate spontaneous ICH.
The CRW stereotactic frame was developed to utilize the existing components of the BRW system. Because of the arc-radius design, this system provides the capability of infinite non-predetermined entry point. This obviates the step of determining entry-point coordinates prior to the target localization which means the simplification of entire procedure. With these characteristics of the CRW head frame, precise localization of hematoma was achieved in spontaneous ICH patients as described above.
CONCLUSION
Spontaneous ICH remains as a fatal and life threatening disease. Because of this character, the need for improved treatment option for ICH is mandatory. Although, there are so many controversies in the treatment of ICH, ICH evacuation using CRW frame would be beneficial in selected patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






