

INTRODUCTION
A typical arteriovenous malformation (AVM) is characterized by abnormal arteries and veins without an intervening capillary bed [1,2]. The resulting hemodynamic instability can often lead to various clinical symptoms, including hemorrhage [3]. Previously, the most appropriate treatment for this condition was surgical removal. However, surgery for AVM was associated with a high risk of postoperative complications.
Following the proven effectiveness of the vascular occlusion mechanism of Gamma Knife radiosurgery (GKRS), the use of GKRS for AVM was introduced at various centers [4,5]. As research progressed, GKRS was established as an effective treatment modality for AVM [6-8]. Subsequent studies also reported on factors that contribute to favorable GKRS outcomes in AVM [9,10].
In particular, several studies have focused on the angiographic features of AVMs. Among these features, the structure of the nidus has been well studied, and the diffuse type nidus was found to be an impeding factor for complete obliteration after GKRS [11,12]. However, the definition of a diffuse type nidus is ambiguous and only a few studies have reported any clarifications. Therefore, further studies are required to determine the effectiveness of GKRS for AVM with diffuse type nidus.
Herein, we analyzed the long-term follow-up results of GKRS for AVM with diffuse type nidus and investigated other factors that may have affected patient outcomes.
MATERIALS AND METHODS
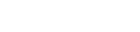
We analyzed 598 patients who underwent GKRS for AVM at our hospital from October 1999 to December 2018. The definition of diffuse type nidus is as follows ŌĆśA lesion with a very unclear margin that diffusely spreads through normal adjacent brain tissueŌĆÖ, referring to previously published study [13] (Fig. 1). Two neurosurgeons examined the patientsŌĆÖ magnetic resonance imaging (MRI) and digital subtraction angiography (DSA) images to make a diagnosis. Any cases of prior surgical treatment were excluded as it may have caused nidus deformation. In total, 75 patients with a diffuse type nidus were included in the study.
Complete obliteration was defined as the absence of a nidus and no venous shunting observable in the patientŌĆÖs DSA. Age, target volume, prescription dose, and the difference in the feeder vessel (single/multiple) were analyzed as factors that could affect obliteration.
For analysis of the nidus, the location was divided into eloquent and non-eloquent areas, and the venous drainage system was divided into either superficial or deep vein. The diameter of the nidus was calculated using MRI T2/time of flight imaging. The volume of the nidus was measured using the GammaPlan 10.1 program.
The linear mixed model test and StudentŌĆÖs t-test were used for the statistical analysis. The Statistical Package for Social Sciences (IBM SPSS ver. 21.0; IBM Corp., Armonk, NY, USA) was used for all calculations, considering a p-value less than 0.05 statistically significant.
RESULTS
Patient demographics
A total of 75 patients were included in the analysis. The mean age of patients was 27.9┬▒17.5 years (range: 4-70 years). The patient group included 38 males and 37 females. The mean follow-up period after GKRS was 67.8┬▒46.3 months (range: 12-206 months). In the initial presentation related to AVM, 50 patients had intracerebral hemorrhage due to AVM rupture (Table 1).
Arteriovenous malformation characteristics
In 18 patients, the nidus was located in eloquent areas, such as the motor cortex and basal ganglia. In 35 cases, the nidus feeder presented with single vessels; two or more feeders were present in the other 40. In 42 patients, the drainage vein in the nidus was the superficial vein, and in 33 patients it was the deep vein. The mean nidus diameter was 20.3┬▒9.8 mm, and the mean nidus volume was 3.3┬▒6.02 cm3 (Table 2).
Gamma Knife radiosurgery profile
The mean target volume was 2.4┬▒2.6 cm3, and the mean prescription dose was 22.9┬▒2.2 Gy. Five patients underwent pre-GKRS embolization. We used a Leksell KULA system (Elekta Instrument, Stockholm, Sweden) until January 2002, after which we used a Leksell Gamma Plan system 10.1.
Clinical outcomes
Among all patients, 34 showed complete obliteration, and the mean time to obliteration was approximately 66 months. Among those with unsatisfactory results after the first GKRS, 28 underwent a second round of GKRS. The mean interval duration to the second GKRS was 51.7 months. Complications included post-gamma bleeding in 3 patients (mean time after GKRS was 12.1 months) and adverse radiation effects in 1 patient (Table 3).
Statistical analysis: complete obliteration rate
Factors affecting the complete obliteration of the diffuse type nidus were analyzed. We analyzed 34 patients with complete obliteration and 41 patients with incomplete obliteration. There was no statistically significant difference between the age profiles of the two groups. The target volume and number of feeders were also not significantly different. The prescription dose for the incomplete obliteration group was 22.1 Gy and for the complete obliteration group was 23.8 Gy, which was statistically significant (Table 4).
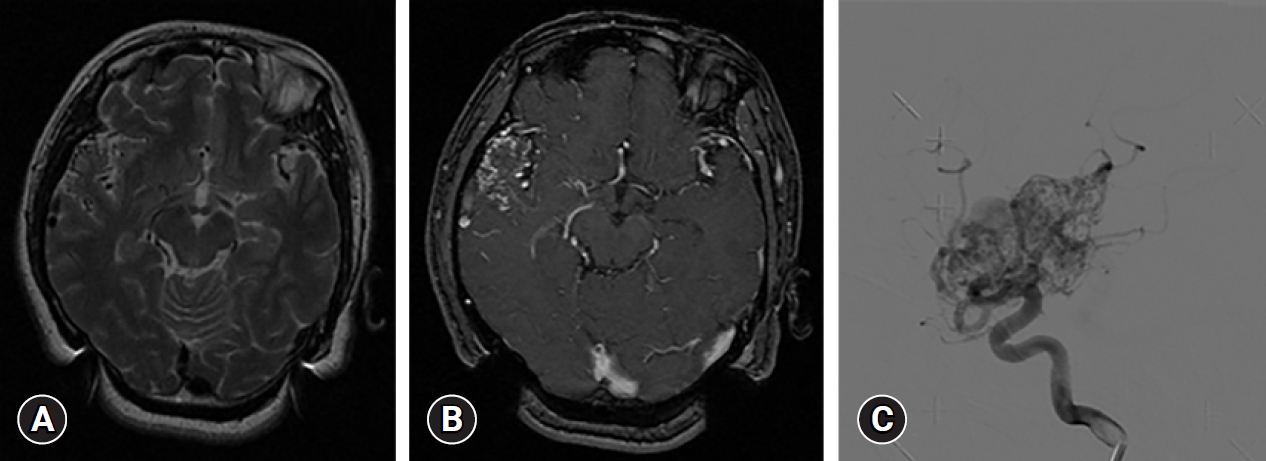
The Kaplan-Meier survival curve for the complete obliteration rate over time showed an overall 5-year obliteration rate of 40% and a 10-year obliteration rate of 70% (Fig. 2).
DISCUSSION
Several previous studies have established the effectiveness of GKRS for AVM [5-7]. In addition, some studies have reported on factors that affect complete obliteration after GKRS. Since AVM is a vascular disease, studies on hemodynamic factors, particularly angiographic features, have also been published [9,10,12].
Zipfel et al. [13] reported that a diffuse type nidus was a risk factor for incomplete obliteration. (Odds ratio=0.25). Further, Chang et al. [14] analyzed the obliteration rate according to the shape of the nidus. These findings indicated that a compact nidus was a favorable factor for complete obliteration. Difficulty in targeting of a diffuse-type nidus is not the only reported reason for a low obliteration rate. According to Meder et al. [15], a diffuse type nidus (sometimes called a non-plexiform nidus) may be insusceptible to complete obliteration due to vascular occlusion because there is a direct arteriovenous fistula in the nidus and an intranidal draining vein. This suggests that even the histological characteristics of a diffuse type nidus affect obliteration.
Another factor that can affect results is the difficulty in targeting a diffuse type nidus [16]. The histopathological structure of a diffuse type nidus is characterized by diffuse lesions around the cortical surface. It also has concurrent focal leptomeningeal angiodysplasia and leptomeningeal vessels with abnormally thickened walls [17]. Therefore, it is difficult to observe a clear nidus using MRI, which is the basis of targeting during GKRS. This ultimately reduces the efficiency of GKRS.
Despite the aforementioned issues, radiosurgery is the preferred treatment for AVM with diffuse type nidus because surgical removal is difficult. Owing to limited treatment options, it is important to develop mechanisms that ensure complete obliteration even in such cases. An appropriate prescription dose was required for complete obliteration in case of the diffuse type nidus. To minimize issues related to GKRS for these cases and to determine an appropriate radiation dose, we ensured the following: 1) The target volume was minimized; staining of the nidus was performed early and angiography was mainly used to target the nidus. Therefore, a sufficient dose of radiation was delivered to the targeted area. 2) The venous structure was excluded when planning the GKRS. This not only reduces the volume of the target, but also helps prevent complications. 3) A treatment plan was prepared using a small collimator with a high isodose profile. Thus, it was possible to minimize the amount of radiation affecting the surrounding brain tissue.
This study has several limitations. First, the definition of a diffuse type nidus is not clear. In this study, the analysis was performed using the radiology classification method, but the diagnosis may have varied depending on the judgement of the examiner. To minimize this bias, a blinded test was conducted by the two radiologists, but no objective classification criteria has been developed yet. Second, complete obliteration was evaluated using only angiography. Although this method is helpful in accurately assessing complete obliteration, there is potential for false negatives in patients who do not undergo angiography.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






