

INTRODUCTION
Navigation refers to a device that indicates the location of an individual and the direction where the individual wants to go. Neuronavigation is the application of navigation to neurosurgery, as information on the location of the lesion and the direction to safely approach the lesion is necessary to improve the surgical outcome. Neuronavigation systems have continued to advance in accuracy and convenience and are now standardized and essential. Neuronavigation provides information on the precise localization and delineation of lesions during surgery using registered images. Such devices are most useful in brain tumor surgery and used in almost all neurosurgical operations. However, since preoperative images are used, neuronavigation does not consider real-time information, and errors may occur during or after the registration step [1,2]. Moreover, if surgeons rely too much on neuronavigation and lack understanding of the systemŌĆÖs principles and errors, surgery may become more difficult. There are two systems of neuronavigation: frame-based system and frameless system. We describe the principles, methods of use, pitfalls, and errors of the widely used frameless neuronavigation system.
CASE REPORT
System (frame-based and frameless system)
The Leksell frame, which is one of the frame-based systems and is commonly used in neurosurgery, was first introduced in 1949. As frame-based systems have high accuracy due to the introduction of computed tomography (CT) and magnetic resonance imaging (MRI), they are mainly used for tumor biopsy and functional neurosurgery, such as procedures for pain, movement disorders, and epilepsy. In frame-based systems, generally, the frame is fixed on the patientŌĆÖs skull before imaging, and the target and trajectory to the target are calculated using the marker shown in the images. A semicircular arc is mounted onto the fixed frame during surgery. However, frame-based systems have several disadvantages, such as patient discomfort during frame fixation and limited visualization of the surgical field.
A frameless neuronavigation system was developed to compensate for the disadvantages of frame-based systems and introduced first in 1986 [3]. These two systems are similar in that they use preoperative images, but frame-based systems analyze the image after the head has been framed. Markers for calculating the trajectory to the lesion already appear on the image, and lesions are recognized and operated through this frame only. However, frameless systems take images without the head being fixated in a frame, so a registration step is required to connect the preoperative images to the actual shape of the patientŌĆÖs head through the fiducials. Frameless systems are widely used and popular because of their good accuracy and ease of use in neurosurgery. And they can also be used for operations requiring high accuracy, such as brain biopsy and deep brain stimulation. So, they are usually used for tumor biopsy and functional neurosurgery. We regularly use the StealthStationTM S8 frameless system (Medtronic Navigation Inc., Louisville, CO, USA) during brain surgery and describe it herein.
Frameless system components
- Optical system (camera, reference frame, tracker, and pointer) (Fig. 1)
- Electromagnetic system (generator, patient tracker, and stylet) (Fig. 2)
How to use
Images and data transfer
Images for neuronavigation are usually collected through CT and MRI. These images must contain fiducials for registration and have enough accurate axial images with a slice spacing and thickness of 1.0 mm. Possible magnetic resonance sequence images include those captured by means of functional MRI, diffusion tensor imaging, and magnetic resonance spectroscopy. Positron emission tomography images also can be used [4]. These images can also be fused onto a reference image to better provide surgical information intraoperatively. These image data are digitalized through the navigation system.
Fiducials
Before scanning preoperative image, the surgeon decides which fiducials to use for registration. There are two types of fiducials with respect to registration. The first is the surface marker used for point-pair registration. There are bone fiducials, anatomical landmarks, and adhesive markers. Bone fiducials are bone screws that are screwed into patientŌĆÖs skull following scalp incision. They confer high accuracy but require an additional scalp incision for their placement. The method of registration through anatomical landmarks uses prominent anatomical points, such as the canthus, tragus, and bridge of the nose. But it is relatively less accurate because of the difficulty in precisely matching each point [5]. The other method involves attaching adhesive markers onto the patientŌĆÖs scalp. It is commonly performed, has reliable accuracy, and is easy to use. However, movement and detachment of the markers cause errors during registration. As different types of adhesive markers are used between CT and MRI, correct markers should be selected carefully. If there are at least four makers adhered to the head, registration can be performed. However, more than 10 markers are recommended because more markers result in higher accuracy and some markers may not be available accidentally. Markers should be widely spaced and distributed evenly on a relatively immovable scalp (Fig. 3). The occipital scalp is more movable than the frontal scalp, so it is not a good location for marker placement because of the possibility for error.
Surface contour is also used for registration. Instead of matching corresponding points from surface markers to the preoperative image, the surface contour method involves scanning the curved surface of the face or head and matching the scanned surface to the preoperative images through multiple random points of the scanned surface [6]. The accuracy of this method is not universal, but this method is easy to use and fast to register [7,8].
Registration
Registration is an essential step in the frameless system. Unlike frame-based systems, frameless systems indirectly recognize the patientŌĆÖs head and lesions through a tracker on the reference frame after imaging. So a spatial relationship between reference frame and the patientŌĆÖs actual head must be established. This step is called ŌĆśregistrationŌĆÖ and is usually executed using the aforementioned fiducials.
There are two methods of registration: point-pair registration using surface markers and surface contour registration. During point-pair registration using adhesive markers, surgeons manually match the markers in the preoperative images and the corresponding adhesive marker on the patientŌĆÖs head one by one. They must be careful not to move and detach the marker, especially during image scanning, the patient moving into the operating room, head positioning, and induction of general anesthesia. If the border or center of the markers is drawn by pen on the scalp immediately after their attachment, moved markers can be easily identified and excluded from the registration step. During head fixation, markers can also move as the scalp is pushed out by head clamping.
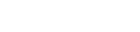
Surface contour registration involves drawing along the curved surface of the patientŌĆÖs face and head with a pointer or laser beam. The system performs the registration step by matching the drawn curved surface to the surface of the head in preoperative images. Including a nose with a prominent curve of the face, a wide head surface area should be used to reduce error (Fig. 4). Areas of movable occipital and compressed temporal scalp that occur during image scanning should not be included for registration.
After registration, the head clamp and reference frame mounted on the patientŌĆÖs head should not be moved because spatial relationships would have already been established between the patientŌĆÖs head and the reference frame. Minimizing errors in the registration step is the most effective way to increase the quality of the frameless system. As navigation systems calculate the distance between corresponding points and display the root mean square error automatically, the extent of error could be checked after registration. About 2 mm of error is generally acceptable. Identifying the anatomical landmarks or surfaces between patient head and preoperative image is one of the manual methods of verifying accuracy.
Device tracking and pointing
Points of interest and trajectories are displayed on the monitor using the pointer. Optical and electromagnetic systems are commonly used tracking methods. In optical systems, the camera emits infrared light to the trackers and recognizes them by reflected light. The pointer is recognized by the system through its mounted trackers and the reference frame. Trackers can be attached to surgical instruments and microscopes, so they can be used as a pointer. This tracking method provides good accuracy, but a free line of sight between the camera and the trackers is needed to keep. If infrared light is blocked by an obstacle and is not reflected by foreign objects on the tracker, such as blood and water, the system does not work.
Electromagnetic systems are based on a generation of magnetic field and the presence of electromagnetic coils in tracking device [9]. The camera and reference frame in optical systems have a similar role to the magnetic field generator and patient tracker. Because this system uses electromagnetic fields, it is not necessary to maintain a free line of sight between the magnetic field generator and patient tracker. Unlike using the patientŌĆÖs head and a fixed reference frame in the optical method, head fixation is not required because the patient tracker is attached on the patientŌĆÖs head and is used instead of a reference frame. As head fixation is not required, this system allows the head to move freely during surgery. The pointer (or stylet) of the electromagnetic system is different than that of the optical system. In optical systems, the pointer is recognized indirectly by a tracker mounted on the opposite side of the pointer tip. However, the pointer in electromagnetic systems is flexible and thin, and recognized directly by the tip of the pointer inserted coil, so it is suitable for catheter insertion because the pointer can be inserted into a catheter. Electromagnetic systems also have some disadvantages. Their accuracy is decreased when the patient tracker moves and detaches. So, patient tracker should be attached at the malar eminence or a relatively immovable area of the scalp and not be moved during head rotation. Large magnetic field generator should also be close enough to the tracker and pointer because the magnetic field is not wide enough, so the surgeon may feel uncomfortable due to generator during surgery. And magnetic substances, including surgical instruments and head clamps, should be kept away from the field of surgery because of the interference caused by ferromagnetic materials [10].
Monitor display
The position and trajectory indicated by the pointer tip are visible on the image within the monitor. Basically, it is possible to see coronal, axial, sagittal, and other planes, such as inline view (along the axis of the pointer) and probe view (perpendicular to the probe axis). The probe view is useful for tumor biopsy and catheter insertion into a lesion. Once the position of interest is specified, the trajectory to that point can be previewed and constructed. The lesion can then be easily and safely accessed while following the trajectory represented by the pointer on the monitor.
Errors and limitations
The most important factor in the use of neuronavigation systems depends on the accuracy of representing the patientŌĆÖs field in the preoperative image; it is important to reduce errors in this process as much as possible. This is due to the fact that neuronavigation systems rely on preoperative images, and this is the most fundamental limitation of such systems.
Some reports have classified and analyzed navigation errors [1,2,11]. Errors can occur during imaging, registration, and operation. Improper image data, such as low resolution, inaccuracy, and magnetic resonance distortion, can be cause of error. Prompt movement or tremor in the patientŌĆÖs head during imaging, wrong marker use, and failure to remove a face mask or hat from the patientŌĆÖs head are other sources of error. Due to these possible sources of error, the registered image must be checked before induction of general anesthesia.
In the registration step, error is related to the fiducials. Regarding the use of adhesive markers, unspaced distribution, low number, movement of the markers, and inaccurate matching of markers can cause errors. When using surface contour, errors can occur due to the difference between the scanned facial surface and the preoperative image, and the location and density of the face curve drawings can affect error.
During operation, the reference frame (or patient tracker in electromagnetic systems) and head can move due to loosing of fixation or carelessness of the surgeon. Because small movement can cause huge error resulting in loss of trust in the navigation system, the surgeon should be very cautious about this. Tight fixation of the head and reference frame is needed, and it is preferable that the reference frame is fixed away from the surgeon to avoid collision by the surgeon during surgery.
Brain shift occurs after the dura is opened and cerebrospinal fluid leaks and its effects are greater due to local tissue deformation when the lesion is removed and the ventricle is opened. Brain shift can be minimized by vertical surgical trajectory, tumor resection in en bloc fashion, and marking the margin of the lesion. Other methods to mitigate brain shift use image update during surgery by intraoperative CT, MRI, and ultrasonography.
DISCUSSION
Frame-based vs. frameless systems
The accuracy of frame-based systems is very high. So, they are usually used for tumor biopsy and functional neurosurgery. With technical advances, tumor biopsy is widely performed using frameless system, and many studies reported no difference in accuracy of diagnostic tumor biopsy [12,13]. And also, no difference in complication rate, operation time and anesthesia time was reported [14,15]. As frame-based systems are limited by spatial restriction and inconvenience for wide opening operations, frameless systems with acceptable accuracy are more desirable for the same operations.
Adhesive marker vs. surface contour
It is generally known that registration using adhesive markers is more accurate than registration using surface contour [16]. However, the registration accuracy using adhesive markers is influenced by the stability of the marker, and the markers are not cost effective because these are disposable. There are many reports that the accuracy of surface contour registration has increased due to technological advances and is comparable to registration using adhesive markers [8,17-19]. Also, in case of surgery without hair shaving, the area to attach the marker is limited. In such instances, surface contour registration is preferable. In prone-positioned operation, both methods are not easy to register without errors. If many markers could be attached widely to the patientŌĆÖs head, adhesive marker is desirable for registration. With respect to registration using surface contour, it can be a little difficult to draw the face of the patient, but it is possible to use this method for same prone-positioned operation with reliable accuracy.
Optical vs. electromagnetic systems
Optical systems using infrared camera cannot be used when infrared rays are obscured by surgical instruments, surgical drapes, or microscopes. Head fixation is also needed to hold the reference frame and head. On the other hand, the biggest advantage of electromagnetic systems is the use of magnetic fields, which eliminate the need to maintain a free line of sight during device tracking. Also, since the tracker is attached to the skin instead of the reference frame, head fixation is not required, so it is useful for surgery that does not require head fixation and requires changes in head position. And electromagnetic systems have comparable accuracy to optical systems [9,20]. So, we usually use this system for intracerebral hematoma aspiration, abscess aspiration, operation of traumatic hemorrhage, ventriculo-peritoneal shunt, and pediatric brain surgery. However, the possibility of tracker movement during operation and magnetic interference is the notable disadvantage of electromagnetic systems.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






