An updated algorithm for the treatment of spinal metastasis
Article information

Abstract
Treatment for spinal metastasis aims to improve patients’ quality of life through specific goals that include improving neurological function, local tumor control, mechanical stabilization, and pain relief. However, various previous strategies have limitations in terms of the application of recent developments in stereotactic radiosurgery (SRS) and minimally invasive spine surgery (MISS), the safety and efficacy of which for spinal metastasis have been well established during the past decade. In this article, we review several previous strategies for the treatment of spinal metastasis and present a new treatment algorithm. This algorithm includes the use of single-fraction SRS and MISS for spinal metastasis. SRS currently offers safe and effective local tumor control in a way that is convenient for patients. Furthermore, MISS (including vertebroplasty, percutaneous pedicle screw fixation, and mini-open decompression) leads to considerable improvements in pain and neurological symptoms with a lower complication rate than conventional open surgery. Based on this new algorithm, patients with spinal metastasis can achieve a better quality of life through fast pain relief, rapid recovery, and minimal discontinuation of chemotherapy. This novel algorithm will enhance patient-centered care in spinal metastasis and can ultimately serve as a simple guideline for spinal metastasis treatment.
INTRODUCTION
As the survival rate of cancer patients improved by the advancement of multimodal treatment, the incidence of spinal metastasis also increased [1]. Major spinal metastasis symptoms include severe axial pain due to pathologic vertebral compression fracture (VCF) and neurological deterioration due to spinal cord compression. Accordingly, treatment of spinal metastasis aims to relieve pain and maintain neurologic function through local tumor control. In other words, the goal of treatment for spinal metastases is to improve the quality of life of the affected patients, not to cure cancer.
It is occasionally difficult to determine the optimal treatment because the clinical conditions of patients with spinal metastasis vary widely. Although several schemes have been developed to assist in treatment decision-making [1-7], there is controversy whether those are the optimal treatment because those could not keep up with recently advanced treatment techniques [8].
Stereotactic radiosurgery (SRS) is an advanced treatment technique that has revolutionized the treatment of spinal metastasis over the past decade due to its being less invasive, simple, and convenient to the patient. SRS has been established as a safe and effective treatment strategy for patients with metastatic spinal tumors owing to its proven therapeutic efficacy [9-11]. Also, there have been significant developments in minimally invasive spine surgery (MISS) since the 2000s. According to the recent literature, MISS for spinal metastasis, such as percutaneous cement augmentation, percutaneous pedicle screw fixation, or mini-open decompression, has demonstrated excellent outcomes of decreased morbidity, quick recovery, and durable pain control [12,13].
The treatment of spinal metastasis requires integrating multidisciplinary approaches involving chemotherapy, traditional surgery, radiotherapy, and new technologies, such as SRS or MISS [8,14,15]. However, previous treatment strategies did not include these new technologies sufficiently. Accordingly, an updated new strategy including advanced technology should be proposed.
In this article, we have systematically summarized the previous treatment strategies for spinal metastasis and proposed a new algorithm to determine the optimal treatment to improve patients’ quality of life.
CLASSIFIED MODEL: TOMITA AND TOKUHASHI SCORING SYSTEM
The treatment strategies for spinal metastasis based on Tomita scoring system [4], Tokuhashi scoring system [3], Baur scoring system [16], Rades scoring system [17], and Linden scoring system [18] are designed to consider patient prognosis, such as life expectancy, and determine the scope of treatment. Classified models and scoring systems allow the physician to predict life expectancy and decide the extent of surgery, but there is a limit to personalized treatment for spinal metastasis. Among these treatment systems, the Tomita and Tokuhashi scoring systems have been considered representative systems and reviewed here.
Tomita scoring system
The Tomita scoring system, introduced in 2001, includes three parameters based on tumor growth, visceral metastases, and the number of bone metastasis lesions (Table 1) [4]. This system intends to help physicians develop an optimal treatment plan based on the predicted patient prognosis. Although the Tomita system helps determine the need or extent of surgery, determining when other treatment options, such as SRS or MISS, should be used is difficult. In addition, this system targets only survival-related prognosis and does not address issues such as improving quality of life, including pain relief and neurological preservation.

A score of characteristics includes parameters based on tumor growth, visceral metastases, and the number of bone metastasis lesions
Tokuhashi scoring system
The Tokuhashi scoring system, similar to the expanded Tomita system, was first introduced in 1990 and revised in 2005 [3]. It is based on six parameters, including the patient’s general condition, location of metastasis, the site of primary cancer, and neurological symptom (Table 2). This system is also designed to help determine the scope of surgical treatment based on the patient’s prognosis. Although the Tokuhashi system provides better predictions than the Tomita system [19], it remains unclear whether it encourages the application of other treatment options, such as SRS and MISS, which improve the quality of life of patients with cancer. Additionally, this system does not consider the contraindications of surgery, such as a cardiac problem or pulmonary dysfunction.

The Tokuhashi scoring system and surgical strategies
MULTIDISCIPLINARY STRATEGIES: NOMS FRAMEWORK, LMNOP SYSTEM, GASBARRINI ALGORITHM, AND SUNNYBROOK PROTOCOL
It has been widely accepted that spinal metastasis is a systemic disease, and its treatment requires the integration of multidisciplinary management. Based on this concept, several multidisciplinary strategies have been developed for optimal treatment. Unlike classified models, these strategies provide a therapeutic method according to individualized patient conditions.
NOMS framework
The NOMS framework is a decision-making scheme developed by the multidisciplinary spine team at Memorial Sloan-Kettering Cancer Center and is designed to facilitate and guide therapeutic decisions [7]. NOMS consists of four fundamental assessments: Neurologic, Oncologic, Mechanical instability, and Systemic disease. The advantage of the NOMS framework is that it incorporates the optimal treatments of SRS, surgery, and systemic therapy. In this framework, the operability depends on the degree of epidural spinal cord compression (ESCC) and the spine’s stability (Table 3). However, this framework does not provide MISS treatment options, such as percutaneous cement augmentation or percutaneous pedicle screw fixation that can improve patients’ quality of life. Also, the treatment tolerability and performance status of the patient is not included in this system. Moreover, the recently emerging chemotherapeutic strategies, such as target therapy and/or immune checkpoint inhibitor treatment, have not been considered in this system; this, therefore, poses a limitation for the continuation of chemotherapy.

NOMS* framework
LMNOP system
Paton et al. [2] have proposed a novel decision-making model called LMNOP that considers critical factors for formulating a management plan while recognizing the individuality of each case. This model considers the tumor location level (L), mechanical instability (M), neurology (N), oncology (O), patient fitness, prognosis, and prior therapy (P) (Table 4). However, this system does not provide a clear therapeutic plan, such as surgery, radiotherapy, or radiosurgery. For spinal metastasis, this system merely lists the circumstances to be considered and does not provide the optimum treatment to be used.

LMNOP* system
Gasbarrini algorithm
The Gasbarrini algorithm, which was proposed in 2002, was also developed considering a multidisciplinary approach for the treatment of spinal metastasis [5]. In this algorithm, operability is regarded as a critical factor in the American Society of Anesthesiology grade. The algorithm provides treatment options for emergency surgery depending on neurological dysfunction and suggests personalized treatment options based on the patient’s status. This algorithm can minimize neurological deterioration and improve local control of tumors (Fig. 1) [20]. However, the major limitation of this algorithm is the lack of treatment options for radiotherapy or SRS.
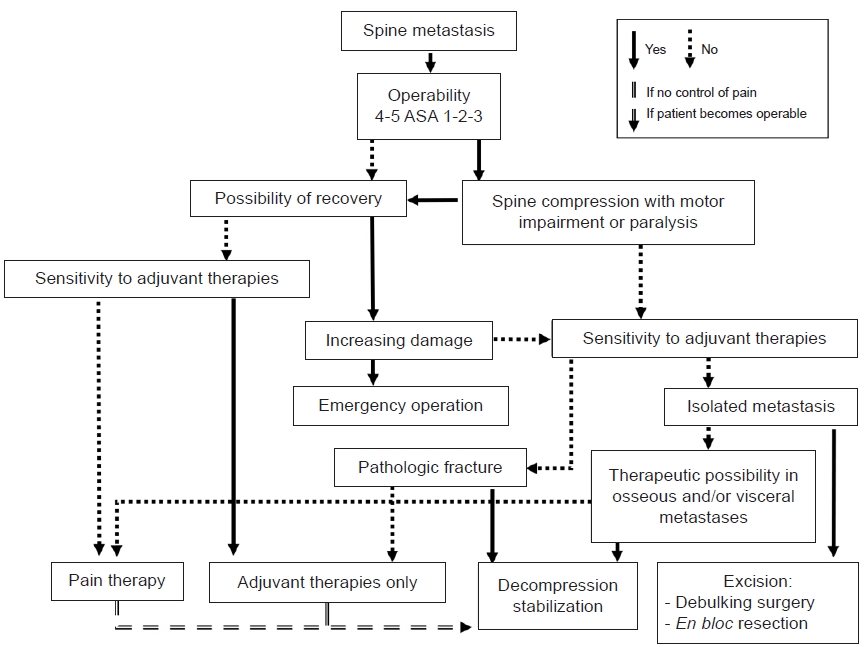
Gasbarrini algorithm for surgical strategy selection. ASA: American Society of Anesthesiology.
Sunnybrook protocol
The Sunnybrook protocol actively utilizes stereotactic body radiation therapy (SBRT) [21]. In this protocol, spinal instability and spinal cord compression determine whether surgery should be performed or whether SBRT or postoperative SBRT should be administered. In the literature, the VCF rate after SBRT has been reported to be 18% of cases, and SBRT >20 Gy increases the incidence of VCF [21]. Based on this concept, the most important step is to assess the risk of VCF after SBRT to avoid neurological deterioration (Fig. 2). However, this algorithm has not performed any oncological assessment, and only the surgical and SBRT aspects have been considered. In other words, multidisciplinary approaches for oncological management, such as tumor biology examination and chemotherapy, have not been made.
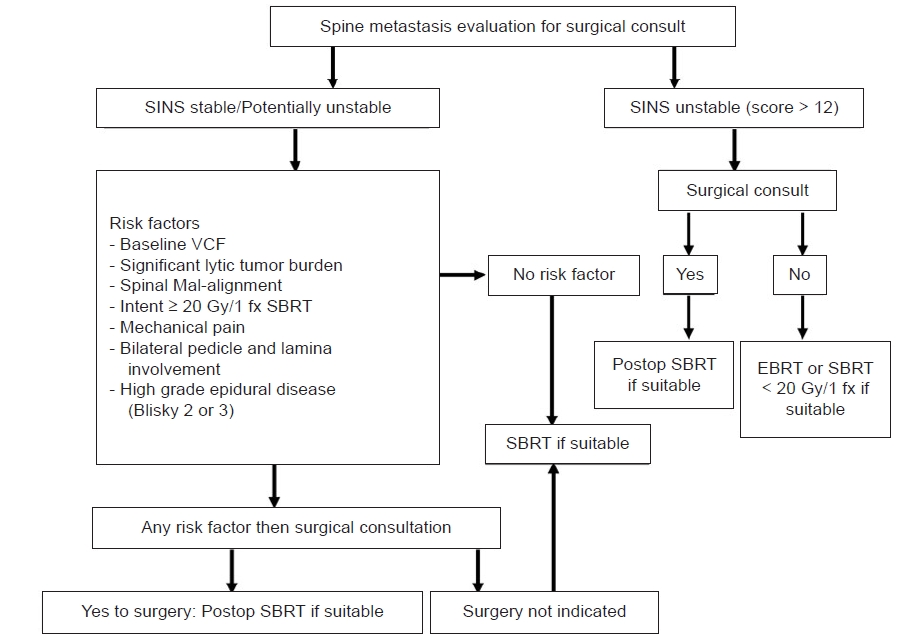
Sunnybrook Odette Cancer Center protocol for spinal metastasis treatment. SINS: spine instability neoplastic score, VCF: vertebral compression fracture, SBRT: stereotactic body radiation therapy, EBRT: external beam radiation therapy, fx: fraction, Postop: postoperative.
NEW STRATEGY FOR SPINAL METASTASIS
The most important considerations of our new strategy for spinal metastasis are as follows.
1. Chemotherapy should be sought as soon as possible because spinal metastasis is a systemic disease. The chemotherapeutic schedule should not be interrupted, if possible.
2. Through SRS and MISS, the patient burden after treatment should be minimized to promote rapid recovery and improve the quality of life.
Our new algorithm is demonstrated briefly in Fig. 3.
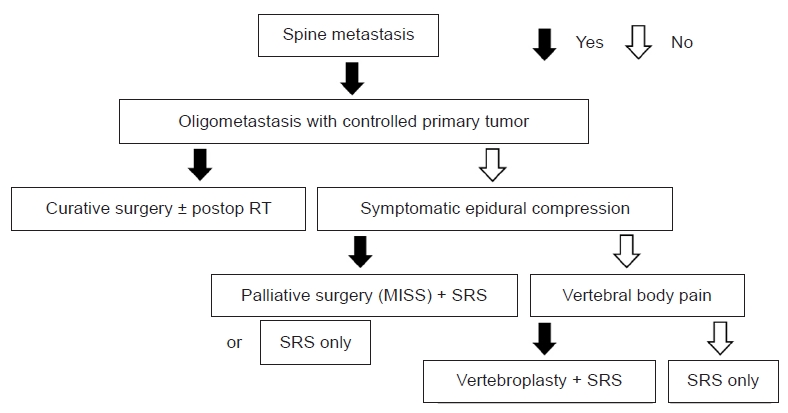
New treatment algorithm for spinal metastasis treatment. Postop: postoperative, RT: radiotherapy, MISS: minimally invasive spine surgery, SRS: stereotactic radiosurgery.
The first evaluation step in patients with spinal metastasis is to assess whether the tumor is progressing, is stable, or is regressing. To this end, we confirm that the tumor is well-controlled and that there is a single- or oligo-spinal metastasis.
If the patient has oligo-metastasis with a well-controlled tumor, extensive curative surgery and/or postoperative radiotherapy of the remnant tumor is recommended. In contrast, neurological symptoms are assessed based on motor weakness and sensory functions if the patient has multiple spinal metastases.
Patients with nerve compression with neurological symptoms may receive palliative MISS, such as percutaneous screw fixation and/or mini-open decompression, following SRS or only receive SRS, depending on their preference or performance status (Fig. 4). By minimizing the scale of surgery, it is hoped that surgical morbidity can be reduced. However, palliative surgery using MISS can be replaced with more extensive surgeries, such as corpectomy and fusion, in selected patients.
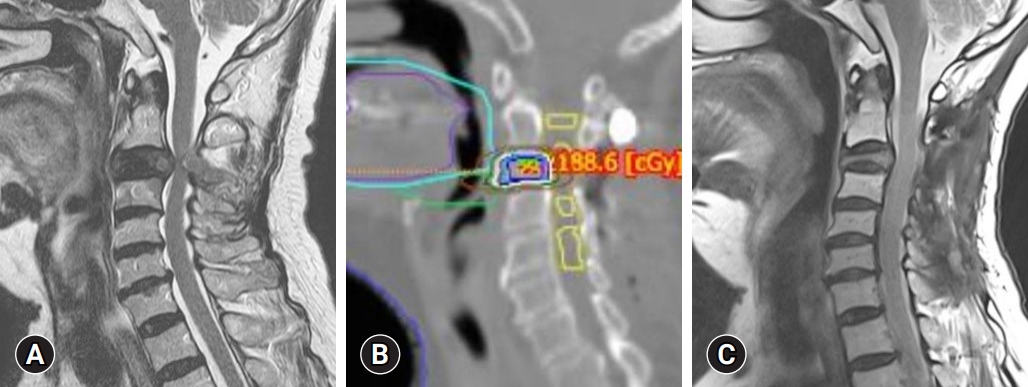
A 73-year-old woman with non-small cell lung cancer presented with severe neck pain and radiculopathy. Cervical magnetic resonance imaging demonstrated a tumor with cord compression at the C3 level. The patient underwent decompressive laminectomy and screw fixation for stability. After surgery, the patient received 18 Gy single-fraction stereotactic radiosurgery. Twelve months post-radiosurgery, she was neurologically intact, had well-controlled disease, and had no pain. (A) Preoperative magnetic resonance imaging demonstrating a C3 tumor with severe cord compression. (B) Radiosurgery was performed using an 18 Gy single fraction. (C) Postoperative magnetic resonance imaging showing circumferential decompression 3 months after radiosurgery.
If the patient does not have neurological symptoms, axial pain due to VCF is considered a criterion for treatment choice. Patients with axial pain and VCF receive vertebroplasty and SRS for rapid pain relief and local tumor control simultaneously. Vertebroplasty is necessary to reduce pain quickly and reduce the risk of progression of compression ratio after SRS. Patients with spinal cord compression without axial pain and VCF can receive SRS only for local tumor control.
The primary concern of single-fraction SRS is the progression of VCF. Some literature has insisted that SRS was correlated to a higher rate of VCF, which is up to 39% after single-fraction of radiosurgery ranging from 18 to 24 Gy [10,22]. Whereas, another study has shown that single-fraction SRS has a similar VCF rate as that of fractionated SRS [23]. In this algorithm, SRS is recommended for patients with ESCC regardless of the presence of axial pain and VCF because the benefits overwhelm the risks in terms of local tumor control and prevention of progression of spinal cord compression.
In this algorithm, the SRS scheme is single-fraction radiosurgery to ensure continuous administration of chemotherapy. Chemotherapy is generally not administrated simultaneously during radiotherapy or hypo-fractionated radiosurgery because of increasing radiation-induced adverse effects. However, single-fraction SRS, high-precision radiosurgery, minimizes damage to normal tissue and allows for simultaneous chemotherapy.
SRS is an effective option in terms of pain and tumor control as 53–95% of patients reported pain relief, and the local control rate was 84–90% [23-27]. Previous randomized trials have demonstrated that SRS for spinal metastasis was associated with a quick improvement of pain than radiotherapy [14]. Furthermore, patients’ quality of life after SRS for spinal metastasis was not worse than that after conventional radiotherapy [28].
Recent advances in MISS have aimed to reduce surgical morbidity while providing favorable neurological improvements in patients treated for spinal metastasis. In a previous study, the complication rate was lower in the MISS group than in the conventional surgery group (17% versus 26%) [15]. However, improvement of pain and the neurological symptom was similar in both groups [15]. Moreover, recently, percutaneous screw fixation without decompression has been suggested for ESCC grade 2 of spinal metastasis as an alternative to conventional open surgery [27]. Regarding this evidence, the MISS is a promising and effective treatment option for patients with spinal metastasis who need surgery.
Of course, our proposed algorithm requires testing in various cases and required verification through clinical trials. Best of our knowledge, this new algorithm is the first to include advanced SRS and MISS in the treatment of patients with spinal metastasis.
CONCLUSION
In the era of prolonged survival among cancer patients owing to advances in chemotherapy, SRS and MISS may improve patients’ quality of life by minimizing the complication or morbidity and allowing minimal chemotherapy delay after SRS or surgery. Although further trial and verification are necessary, our simple strategy may benefit patients who are either surgical candidates or need systemic treatment for their spinal metastasis.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.