

INTRODUCTION
Blepharospasm is a disease in which the closure rate of the bilateral eyelids increases, mainly due to involuntary contraction of the orbicularis oculi, procerus and corrugator muscles [1,2].
Blepharospasm, oromandibular dystonia, and Meige syndrome are different from each other but closely related. Meige syndrome is characterized by combination of cranial involvement, includes blepharospasm and involuntary oromandibular dystonia movement. Most researchers and clinicians believe that Meige syndrome, blepharospasm, and oromandibular dystonia are not one single entity, but a multi-factor origin clinical syndrome [3].
Medical treatment of these conditions has generally been unsuccessful and limited due to adverse side effects [3]. Although, botulinum toxin has been shown to be effective for many dystonic features including blepharospasm, many patients show diminished response over time [4,5]. Some patients become resistant to continuous treatment because antibodies develop [5]. To treat these disease surgically, stereotactic ablation techniques targeting the thalamus or the globus pallidus interna (GPi) have been used for several years with variable results [6-10].
The Application of deep brain stimulation (DBS) to various movement and nonmovement disorders has increased interest in the treatment of severe forms of medically refractory dystonia. In particular, the GPi was an effective target for primary generalized dystonia [11-15]. There have also been several reports of the good efficacy of GPi DBS for craniocervical dystonia or Meige syndrome [16-23].
Blepharospasm can be the most incapacitating symptom, whether focal or part of Meige syndrome. There have been rare case reports of using GPi DBS for pure blepharospasm [24,25].
The objective of this study was to report our results about postoperative outcome after DBS in total of 10 cases of pure blepharospasm after at least 12 months follow-up.
MATERIALS AND METHODS
Patients
Ten patients with pure blepharospasm who underwent GPi DBS at The Catholic University of Korea, Incheon St. MaryŌĆÖs Hospital between 2019 and 2021 were included in this study. All patients were evaluated by movement disorders specialists composed of neurosurgery, neurology and rehabilitation medicine team at our center. The patients suffered severe disease-related functional impairment with unsatisfactory outcomes after oral pharmacotherapy, which included the use of benzodiazepines, anticholinergic agents, antispasmodic agents, and antiepileptic agents. All the patients also showed poor response to botulinum toxin injections. Five patients also tried some alternative therapies including physical therapy and acupuncture. Brain magnetic resonance imaging (MRI) demonstrated no structural lesion as a possible cause for their dystonia. Preoperative and postoperative Burke-Fahn-Marsden dystonia rating scale (BFMDRS) movement subscale (BFMDRS-M) scores (range 0-120), Blepharospasm Disability Index (BSDI, range 0-24), and Jankovic Rating Scale (JRS, range 0-8) were counted for each patient at 6 months and over 1 year after surgery.
Ethical statements
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Catholic Medical Center at the Catholic University of Korea (IRB approval No. OC18RESI0108). Informed consent was obtained by all subjects when they were enrolled.
Statistical analysis
Statistical significance of changes in clinical rating scales at 6 months and over 1 year compared with baseline was assessed using the Wilcoxon signed rank test (paired). A significance threshold of 0.05 was used, and all analyses were conducted using IBM SPSS Statistics 25 (IBM Corp., Armonk, NY, USA).
Surgical procedures
All surgical procedures were performed under general anesthetics. The GPi was used for DBS target. Based on anterior and posterior commissures, initial GPi coordinates were 3 mm anterior and 3 mm inferior to the midcommissural point and 22 mm lateral to the mid-line. In addition to the above indirect targeting measures, direct targeting was implemented based on MRI performed on the day of surgery in an attempt to compensate for individual variations. We established entry/target points and the entire trajectory using planning software (Medtronic Stealthstation Planning software; Medtronic, Dublin, Ireland) to avoid the sulci, ventricle, and vessels along the trajectory. For the GPi, the trajectory was planned to be lateral to the ventricle, traverse the posterior GPi, and terminate above the optic tract. In the operative field, we usually placed the burr hole about 0.5-1 cm anterior to the coronal suture and 3.5-4 cm from the midline. Microelectrode insertion was done 3 mm above the target using three concentric bipolar tungsten microelectrodes (central, anterior, lateral) driven simultaneously by an Elekta MicroDriveTM (Elekta, Stockholm, Sweden) at incremental depths of 0.5 mm until 2 mm above the target and then 0.2 mm in depth. Intraoperative electrophysiology was performed using a LeadPoint system® (Medtronic, Tokyo, Japan) to locate and confirm GPi neuronal activity. Medtronic® 3389 quadripolar (Medtronic, Minneapolis, MN, USA) or Abbott® (Abbott Neuromodulation, Austin, TX, USA) or Boston scientific® directional electrodes (Boston Scientific, Marlborough, MA, USA) were implanted bilaterally. At a subsequent surgery, DBS electrodes were connected to an implantable pulse generator. Postoperative nonenhanced brain computed tomography imaging was performed to confirm the accuracy of electrode placement in the GPi and check postoperative complications such as intracerebral hemorrhage.
RESULTS
Clinical characteristics and individual demographic profiles of patients are summarized in Table 1. The median age of patients at surgery was 56.5 years (interquartile range [IQR], 50.5-65.8 years) and the median length of time from disease onset to the time of surgery was 58.0 months (IQR, 46.8-64.3 months). The median postoperative follow-up period was 22.5 months (IQR, 15.3-29.0 months).
Preoperatively, all the patients received medical treatments for management of their symptoms. Seven patients received benzodiazepines. One received antispasmodic drugs (baclofen). One received antiepileptic agents (topiramate). One received Gabapentin. Two received other agents such as muscle relaxant. Two received antidepressant agents (selective serotonin reuptake inhibitor, selective serotonin noradrenalin reuptake inhibitor). Eight of 10 patients (80.0%) received multiple drugs combination for managing their symptoms. All patients had an alternative treatment history with botulinum toxin injections before surgery. At the last follow-up, although all the patients were continuing medication, there was a decrease in the number or doses of medications in three of eight patients who were taking multiple drugs.
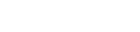
In terms of postsurgical outcome, The median of BFMDRS-M scores at the three time points (preoperative baseline, 6 months, and over 1 year of follow-up) were 7.0 (IQR, 6.0-8.0), 4.5 ([IQR, 3.9-6.0], 35.7% improvement, p<0.001), and 3.8 ([IQR, 2.8-5.3], 45.7% improvement, p=0.002), respectively (Table 2, Fig. 1). Of all patients, one showed substantial improvement in symptoms (over 80% of BFM improvement at the last follow-up). Five patients showed the best benefit at a short-term interval as well (Table 2). As compared with baseline values, the majority of movement subscores had decreased at month 6 and remained stable for over 1 year.
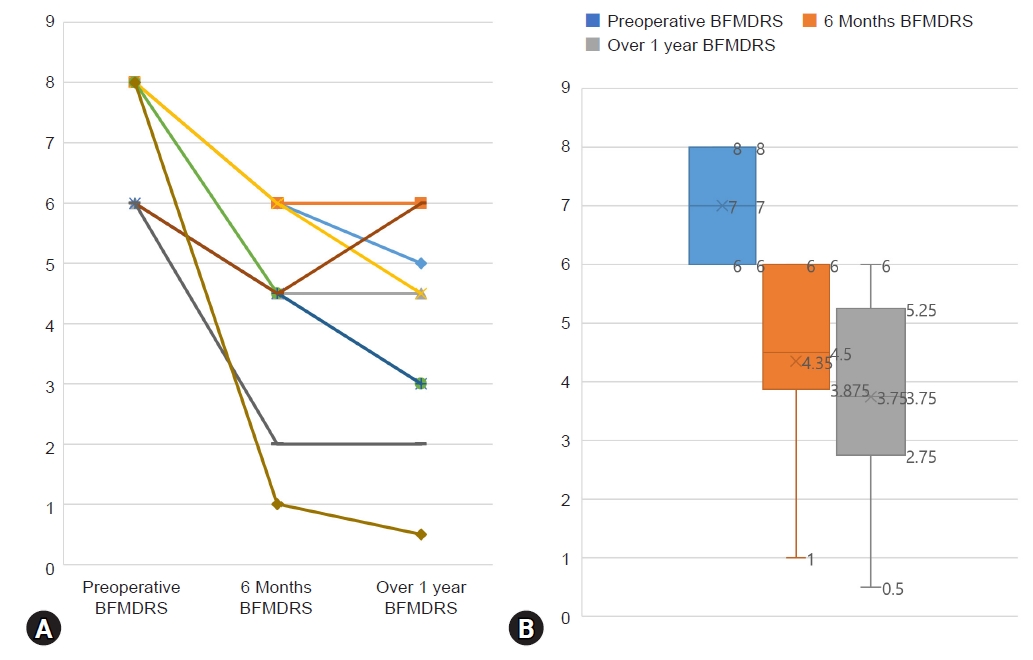
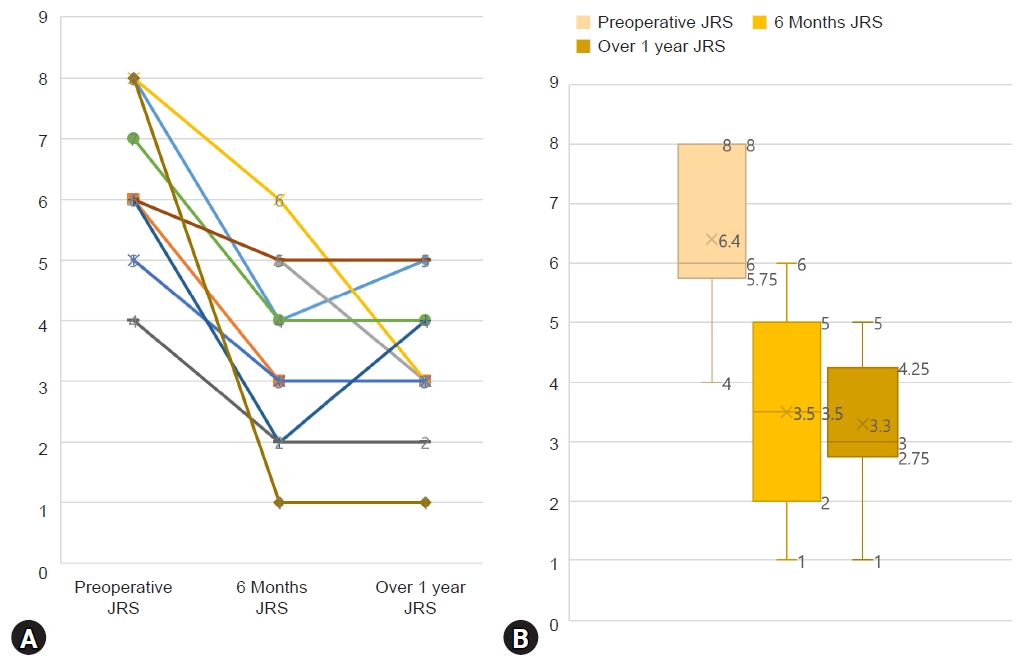
At the three time points, BSDI and JRS were checked as well. Similar to results of BFMDRS-M, improvement rate of JRS was 41.7% (p<0.001) and 50.0% (p<0.001) at 6 months and over 1 year after surgery, respectively. However, improvement rate of BSDI was 54.8% (p<0.001) and 61.3% (p<0.001) respectively for 6 months and over 1 year, slightly better than BFMDRS-M and JRS improvement rates (BSDI in Table 3, Fig. 2; JRS in Table 4, Fig. 3). All 10 patients who participated in our study had no postoperative complication such as hemorrhage and infection. There are summarized each scales and improvement rates in Table 5.
Stimulation parameters for the 10 patients are presented in Fig. 4. Of a total of 20 electrodes implanted in these 10 patients, nine patients were on a monopolar stimulation, and the rest one patient was on a bipolar stimulation at the last follow-up. The median voltage or current was 3.93 V (IQR, 3.63-4.18 V) (or mA) on the left and 3.80 V (IQR, 3.63-4.06 V) (or mA) on the right. All patients showed a stimulus intensity of more than 3 V in amplitude. The median pulse width was 75.0 μsec (IQR, 60.0-90.0 μsec) on the left and 80.0 μsec (IQR, 62.5-90.0 μsec) on the right. The median frequency was same value as 174 Hz (IQR, 162.5-180 Hz) in both sides. Six out of 10 patients were implanted using directional lead manufactured by Boston scientific® or Abbott®.
DISCUSSION
Terms of blepharospasm, oromandibular dystonia, and craniocervical dystonia are used to describe a focal or segmental dystonia whereby involuntary contraction of facial, masticatory, lingual with or without cervical muscles result in sustained and forceful movement of the related musculature. As a group of conditions that can affect the motor aspect of eye, upper and lower face, mouth and hypoglossal cranial nerves, pure blepharospasm is an uncommon disease. It is easy to make a wrong diagnosis as it can resemble symptoms of many other facial movement disorders such as hemifacial spasm, tremor, tic, chorea, and stereotypies [26]. Therefore, the diagnosis of blepharospasm can be challenging. A lot of factors including patientŌĆÖs physiologic and psychological status and the clinicianŌĆÖs training can affect an accurate diagnosis at the time of presentation.
Since Vercueil and coworkers [27] first reported the outcome of a bilateral GPi DBS in a patient with Meige syndrome, several studies have reported that the segmental dystonia responds to GPi DBS [28-37]. However, there were only three studies on the usefulness of GPi DBS in ŌĆ£pureŌĆØ or ŌĆ£isolatedŌĆØ blepharospasm, and even that were single case studies [24,25,38]. Our study included the largest number of patients among studies reported up to date.
According to Ostrem et al. [13], six cases with cranial-cervical dystonia showed a mean improvement rate of 86% based on the BFMDRS eyes score at 6 months postoperatively compared to baseline. Similarly, Sako et al. [33] described five patients with MeigeŌĆÖs syndrome who experienced 88% improvement of BFMDRS eyes score. Meanwhile, according to Reese et al. [39], 12 patients with Meige syndrome for up to 78 months after bilateral GPi DBS showed a mean eyes improvement rate of 38% after a short-term follow-up (4.4┬▒1.5 months; p<0.001) and a rate of 47% after a long-term follow-up (38.8┬▒21.7 months; p<0.001). Although our study was focused on pure blepharospasm, their result appeared to be similar to ours.
Santos et al. [25] reported in 2016 the first case of pallidal stimulation successfully done on pure blepharospasm, with 63% improvement rate of JRS score. This was soon followed in the same year by the report of Yamada et al. [24] of pure blepharospasm responding to bilateral pallidal DBS, with 87.5% improvement of BFMDRS score, 91.7% improvement of JRS score, 100% improvement of BSDI score, respectively. Evidente at al. [38] also reported the outcome of bilateral pallidal DBS for pure blepharospasm, with results of 100% improvement of BFMDRS and JRS score at 30 months. However, while those were all single case reports, our study is meaningful in that more patients are included.
In our study, one of patients (10.0%) had an improvement of more than 80.0% and four patients (40.0%) had 50% to 80% improvement rate compared to their baseline scores in terms of BFMDRS-M. The benefit was also sustained over the course of the last follow-up (until June 2022), although it waxed and waned depending on the patientŌĆÖs condition at the day of the visit to the outpatient clinic. The results of BFMDRS-M and JRS scores were somewhat similar, but BSDI was slightly better than the others. BSDI is a quality of life form written by the patient oneself, but the other scorings are form in which the patient comes to the hospital and evaluated by the medical staff. Therefore, it is possible that the symptoms that the patient usually feels in daily routine are evaluated better than the other scores.
Moreover, the postoperative outcome could be affected to genetic or individual heterogeneity [15], and how appropriately the operation was carried out. In perspective of the operation process, the specific type of dystonia, the choice of the target, the anatomic location of the electrodes, and technical or human error during the procedure all could influence the therapeutic outcome [40-42]. Besides, various factors such as postoperative patientsŌĆÖ physiologic and psychologic status, inappropriate stimulation method applied during postoperative outpatient visit could limit favorable outcome. According to Wang et al. [43], Four factors such as 1) the DBS target (subthalamic nucleus vs. GPi); 2) whether symptoms first appeared at multiple sites or at a single site; 3) the subitem scores of the mouth at baseline; and 4) the follow-up period could affect significant differences between the good and poor outcome after DBS of primary Meige syndrome. Although we have yet to find predictive factors affecting the outcome, large-scale, prospective, randomized clinical trials and electrophysiological or neuroradiological studies are warranted in the future.
This study has several limitations. First, it was retrospective in nature and the outcome was collected by an unblinded rater. In addition, measures for dystonia disability scale in BFMDRS such as speech, handwriting, feeding, eating/swallowing, hygiene, dressing, and walking were not carried out. Although this should not cause a serious bias, it might have an impact on estimating the effectiveness of the treatment.
CONCLUSION
Bilateral GPi DBS in pure blepharospasm can be effective if conservative treatment options fail. The benefit is not only observed at a short-term follow-up period, but also maintained at a long-term follow-up. While no definitive risk factors affecting favorable outcome are yet to be made for pure blepharospasm, further studies in the future could clarify possible predictive factors affecting favorable outcomes. Results of this study along with those of other reports suggest that bilateral GPi DBS might be an effective treatment for medically refractory pure blepharospasm even in a long term.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






