

INTRODUCTION
Schwannoma is the most common tumor of peripheral nerve, which originate from Schwann cells around axons of motor and sensory neurons [1]. Typically, they are painless, slow-growing, isolated, firm and round laterally movable masses [2]. Patients with a peripheral nerve schwannoma may exhibit TinelŌĆÖs sign which is the paresthesia in the distal distribution of the affected nerve upon tapping. In the periphery, it occurs more commonly in the upper extremities than in the lower extremities, and among them, sciatic schwannomas are rarely reported [3,4]. In addition, approach to the sciatic nerve is not familiar to neurosurgeons because it is not a common site for nerve entrapment syndrome or injury.
In this article, we report a patient whose schwannoma was successfully enucleated in the midportion of the sciatic nerve guided by the intraoperative nerve stimulation, focusing on the technical and anatomical aspects of surgery.
CASE REPORT
A 62-year-old male presented with palpable mass in the right posterior upper thigh, just below the gluteal fold. The mass had been continuously growing for 3 years and reached the size of a tennis ball. At first it was asymptomatic, but after 2 years, the patient began to feel dull pain around the mass. He had no history of benign or malignant tumors anywhere else on his body and had no cafe╠ü au lait macules. On physical examination, the mass was firm and movable only in the lateral direction to the sciatic nerve. TinelŌĆÖs sign was negative. He showed no neurological symptom or sign with all motor and sensory functions preserved in the right leg. Magnetic resonance imaging showed about 9-cm-sized encapsulated solid mass in the middle of the sciatic nerve, just beneath the biceps femoris muscle. It was isointense to nearby muscles on T1-weighted images, and hyperintense on T2-weighted images with heterogenous contrast enhancement (Fig. 1). Considering continuous growth of the mass, and aggravating discomfort in the thigh, surgical removal of the tumor was planned.
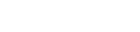
Surgery was performed with the patient in prone position. Total intravenous anesthesia using propofol and remifentanil was applied for intraoperative nerve stimulation and electromyography (EMG) monitoring of distal muscles. Rocuronium, the muscle relaxant, was used only for endotracheal intubation and then stopped immediately. Stimulation induced EMG waveform recording was prepared in gastrocnemius muscle for tibial nerve and in tibialis anterior muscle for common fibular nerve. In addition, transparent surgical drape was used for visual observation of stimulation induced distal muscle contraction (Fig. 2A).
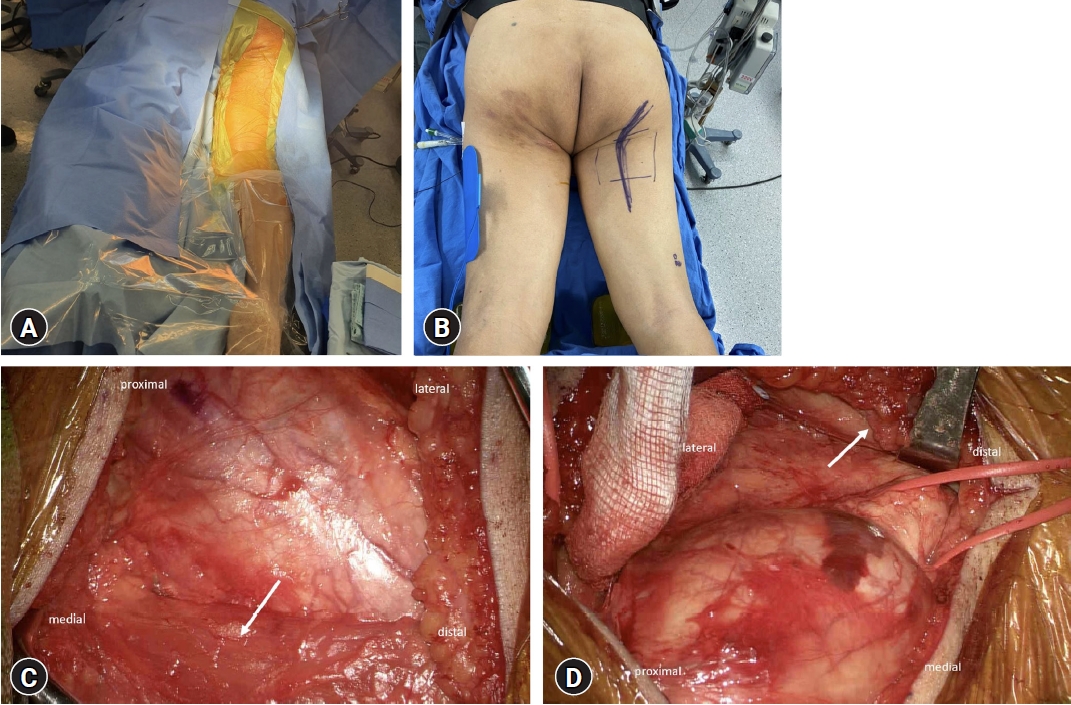
We made a vertical skin incision on the middle of the palpable mass with laterally curved upper end to the inferior gluteal region (Fig. 2B). The tumor was located just deep to the biceps femoris and gluteus maximus, and was compressing the biceps femoris, making it thin and wide. We exposed the tumor-bearing sciatic nerve from the proximal 3 cm to the distal 3 cm. Proximally, sciatic nerve was revealed by retracting the gluteus muscle upward and the biceps femoris muscle to medial direction (Fig. 2C). However, the biceps femoris muscle should be retracted to lateral direction when we obtained the sciatic nerve distal to the tumor (Fig. 2D). We could avoid excessive muscle stretching by retracting the biceps femoris medially and laterally as needed.
After exposing the whole tumor, the proximal and distal sciatic nerve circumferentially, we stimulated the surface of the tumor to find the ŌĆśsafe zoneŌĆÖ, the area that fascicles are widely splayed apart, suitable for beginning dissection [5]. A stimulating electrode was applied on the surface of the tumor with 5 Hz, 2 mA stimulation. Any distal muscle contraction, detected by the EMG recording or by visual observation, were marked on the tumor surface (Fig. 3). A safe dissection zone was established, and the tumor was carefully dissected from the traversing fascicles. Internal neurolysis was performed using microsurgical technique to find the one fascicle entering and exiting the tumor (Fig. 4A, B). Stimulation of the fascicle showed no distal muscle contraction and then coagulated. The 9.0├Ś6.0├Ś3.5 cm tumor was successfully enucleated with each proximal and distal tumor related nerve fascicles ligated (Fig. 4C). It was histologically confirmed as schwannoma.
The postoperative course was uneventful. All motor and sensory functions of the right leg was preserved until the last follow-up day, 6 months after surgical removal.
DISCUSSION
Most patients with peripheral nerve schwannoma have intact neurological function because they grow slowly, elongating the fascicles of affected nerve [1,6,7]. Therefore, successful surgical removal of a peripheral schwannoma must meet two requirements. The first is complete tumor removal without remnant tumor cells, and the second is a safe operation that preserves preoperative neurological functions as much as possible.
Since the middle portion of the sciatic nerve is not a location where nerve entrapment syndrome commonly occurs, the surgical approach is not familiar to neurosurgeons, and it is difficult to find detailed techniques in the literature [4,8]. Because the tumor in this patient was large, sufficient proximal and distal exposure including the middle portion of the sciatic nerve was required. When removing the patientŌĆÖs tumor, damage to the connective tissue could be minimized with an appropriate anatomical approach, and functioning nerve fascicles could be preserved as much as possible through intraoperative neurostimulation-guided dissection. The following three factors were essential for surgical removal of this patientŌĆÖs tumor safely and effectively.
Exposing the middle portion of the sciatic nerve
We made a vertical skin incision in the posterior aspect of upper thigh, on the middle of the palpable mass, with laterally curved upper end to the inferior gluteal region (Fig. 2B). This incision facilitated direct access to the tumor in the middle portion of the sciatic nerve and was useful for securing the proximal sciatic nerve by lifting the gluteus maximus muscle. Access to the pyriformis muscle, which can cause entrapment syndrome of the proximal sciatic nerve, is possible through the transgluteal approach [9]. However, in this patient, access to the distal portion rather than the location of the pyriformis muscle was required, and simultaneous exposure of the upper and middle sciatic nerves was required. Therefore, we retracted the gluteal muscle in an upward direction, which helped to minimize the muscle injury that could occur in the transgluteal approach and provided sufficient visual field for surgery.
Retracting direction of biceps femoris muscle
To successfully remove the peripheral nerve schwannoma, the proximal and distal portions of the nerve, including the location of the tumor, must be secured [10-12]. In this case, the tumor was located just beneath the long head of the biceps femoris muscle and was compressing and thinning the muscle. Therefore, in order not to separate the biceps femoris, it was necessary to be retracted laterally or medially. In the proximal area of the thigh, the tumor and proximal sciatic nerve were exposed only when the biceps femoris long head was retracted in the medial direction (Fig. 2C). However, when the biceps femoris was retracted to the medial, the distal portion of sciatic nerve to the tumor could not be observed or excessive muscle retraction was inevitable which could lead to serious muscle damage. The distal sciatic nerve could be easily secured by retraction of the biceps femoris in the lateral direction, which is opposite to the direction of muscle retraction for exposing the proximal sciatic nerve (Fig. 2D). We could easily perform neurolysis at the proximal and distal end of the neurogenic tumor through this retraction method, and prevent surgical complications related to excessive muscle damage.
Intraoperative neurostimulation-guided internal neurolysis
Advances in intraoperative neurophysiological monitoring (IONM) have greatly contributed to the safety of brain and spine surgery, as to peripheral nerve surgery. In neurosurgery, it is important to monitor the integrity of the nervous system from central to peripheral. While most of IONM technique shows damaged nerve function after manipulation, in peripheral schwannoma surgery, however, it helps to determine which area to avoid dissection to prevent nerve damage before manipulation. We stimulated the surface of the tumor to find the ŌĆśsafe zoneŌĆÖ, with a stimulating electrode. Stimulation induced EMG waveform was monitored in gastrocnemius muscle and in tibialis anterior muscle (Fig. 3) [5,13]. Additionally, visual observation and palpation of the distal muscles enhances the effectiveness of detecting stimulation-induced muscle contractions. We applied the transparent drape in lower leg that helped to visually detect the contraction of the distal muscles while keeping the surgical field sterile (Fig. 2A). Through the marked safe dissection plane, the tumor was safely removed from the sciatic nerve proper.
CONCLUSION
Understanding the relevant anatomy and retracting the biceps femoris long head to an appropriate direction helped us remove a large schwannoma in the middle portion of sciatic nerve, minimizing muscle damage. The use of intraoperative nerve stimulation-guided tumor dissection was useful to preserve viable fascicles of parent nerve.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






