

INTRODUCTION
Fahr disease, also known as idiopathic basal ganglion calcification (IBGC), is a rare and genetically heterogeneous neurological disorder that remains poorly understood [1,2]. It is characterized by abnormal calcium deposits in certain brain regions, mainly the basal ganglion. To date, the mechanism underlying the formation of these deposits remains unlcear. Although a genetic component associated with this disease exists, the specifics of inheritance and the involved genes still needs clarification.
Fahr disease was named after the German pathologist Karl Theodor Fahr who first described the condition in 1930 [3]. The term “idiopathic” is used to describe a disease or condition with an unknown or unclear origin, which reflects our current understanding of Fahr disease.
Bilateral basal ganglion calcification is a typical feature for diagnosing Fahr disease; however, an additional calcification detected in other areas is difficult to distinguish from brain lesions accompanied by calcification. We herein report an interesting case of Fahr disease with multiple cerebral calcifications requiring a differential diagnosis from cerebral cavernous malformation (CCM) or brain tumor.
CASE REPORT
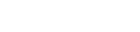
A 63-year-old woman was referred to our hospital from a local clinic for further examination. She had visited the clinic for intermittent dizziness with no other neurological symptoms. She had been initially diagnosed with CCM or brain tumor with physiological basal ganglion calcification. No symptom of cognitive impairment, or movement disorder, or any focal neurological deficits were observed before admission. The results of neurological examination were unremarkable, and there were no unusual findings in the family history. Initial brain computed tomography (CT) showed multiple calcified lesions in both basal ganglia, both cerebellar hemispheres, and the left frontal lobe (Fig. 1). Brain magnetic resonance imaging (MRI) revealed no prominent lesions on T2- and T1-weighted image, and there was no contrast enhancement after gadolinium injection. However, multiple low signals were seen on gradient echo MRI (Fig. 2). Furthermore, dense dark signals were observed in both basal ganglia and mild dark signals in the right cerebellar hemisphere and left frontal lobe. The calcified lesions were much more visible on brain CT than on MRI. The presence of these lesions initially suggested CCM or calcified brain tumor with concurrent physiological basal ganglion calcification, as basal ganglion calcification was considered a common finding whereas calcification in other sites a rare finding. Further investigations, including a detailed review of imaging findings and clinical features, led to diagnosis of Fahr disease. This diagnosis was made after knowing that calcifications could come in other forms besides bilateral basal ganglion calcifications. The patient did not receive special treatment but was planned to undergo follow-up to the potential development of neurological symptoms in the future.
DISCUSSION
Fahr disease, also known as IBGC, is a rare neurological condition of unknown etiology; it is characterized by the presence of bilateral calcification in the basal ganglion [1,2]. Its clinical presentation varies, often involving a broad spectrum of neuropsychiatric symptoms. This highlights the diagnostic challenges associated with Fahr disease. The rarity of this condition and the wide variety of its clinical presentations often render accurate diagnosis difficult. Furthermore, it can be easily overlooked in favor of more common conditions with similar symptoms or imaging findings. The lack of a clear genetic marker or definite diagnostic test further complicates the diagnosis. Recently, genetic mutations for Fahr disease have been described in SLC2042, PDGFB, and PDGFRB [4,5]. We believe that these findings will improve our understanding of the pathophysiology of this disease and significantly contribute to the future development of treatment. These genetic mutations identified so far have different pathogenic mechanisms. These points suggest that Fahr disease is not a monogenic disorder and that several mechanisms of calcium or phosphate transport contribute to the end result of brain calcification.
Fahr disease refers to idiopathic calcification of basal ganglion without a secondary cause. Basal ganglion calcification mainly caused by physiological and metabolic factors, idiopathy, toxicity, radiation therapy, infection, birth hypoxia, and heridity. These causes should be excluded in the diagnosis of Fahr disease.
The clinical presentation of Fahr disease can widely vary among patients, ranging from neuropsychiatric symptoms, such as cognitive impairment, psychosis, and mood disorders, to more neurological symptoms, such as movement disorders and seizures. The age of onset can also vary and in some cases, patients may remain asymptomatic.
The main radiologic tool for the diagnosis of Fahr disease is CT scan, which is known to be more sensitive than MRI. The most common finding is calcification of the basal ganglion, including the globus pallidus, thalamus, and dentate nucleus in a symmetric pattern. Other less commonly reported areas of calcification include the brainstem, cerebellum, and cortical and subcortical white matters [6]. In our case, which is bilateral basal ganglion calcifications, dentate nucleus were found, but asymmetric calcifications were also observed in the frontal lobe, which is uncommon. Furthermore, the cerebellar lesions that were prominent on CT were not prominent on MRI. Diagnosis this disease with MRI alone is challenging. The degree of density and symmetry of calcification may be associated with the degree of disease progression. Usually, physiological calcification in the basal ganglion is confined to the globus pallidus, is both sides, and faint, and other calcifications are often found in pineal gland, falx, arachnoid granulation, and choroid plexus. However, if the calcifications are dense, involve the thalamus bilaterally and dentate nucleus, and occur in the cerebellum, brainstem, and cortical and subcortical white matters, Fahr disease should be suspected [7]. In people aged below 40 years, a secondary cause almost frequently exists [8]. Through the history, drug, poison, CNS infection, radiation exposure should be ruled out. Parathyroid disorder, which is an important cause of intracranial calcification, can be diagnosed through blood tests.
It is crucial for clinicians to consider Fahr disease in patient presenting with multiple cerebral calcifications. Although the patient history, clinical presentation, and imaging findings are all significant, none of these alone can help in the definite diagnosis of Fahr disease. However, a combination of all these elements will be able to confirm a presence of this disease.
CONCLUSION
Fahr disease is rare but significant neurological condition that requires careful consideration during diagnosis, particularly in patients presenting with multiple cerebral calcifications. Detailed history, comprehensive clinical evaluation, and thorough imaging review are crucial in making at the correct diagnosis, thereby preventing unnecessary invasive procedures or treatments. Our case highlights the educational importance of Fahr disease as a differential diagnosis when evaluating brain lesions with multiple calcifications.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






