

INTRODUCTION
Trigeminal neuralgia (TN) is an oro-facial pain along the trigeminal nerve dermatomes. It can be idiopathic, classic, or even secondary to the space-occupying lesion such as vestibular schwannomas, cerebellopontine angle (CPA) meningiomas. Stereotactic radiosurgery (SRS) including Gamma Knife radiosurgery (GKRS) has emerged as a treatment option for secondary trigeminal neuralgia (STN) because of its non-invasiveness and low risk of complications. Favorable outcomes of SRS for TN secondary to benign tumor have been consistently reported [1,2]. But SRS has certain drawbacks, including a relatively long time to achieve symptom relief, without surpassing the clinical outcomes of surgical resection. Previous studies have reported that it takes approximately 5.7 to 10.5 months for pain reduction following GKRS [1]. This case report presents a patient with STN who underwent two GKRS sessions but experienced no pain relief. Ultimately, surgical resection was performed 2 years after the initial diagnosis.
CASE REPORT
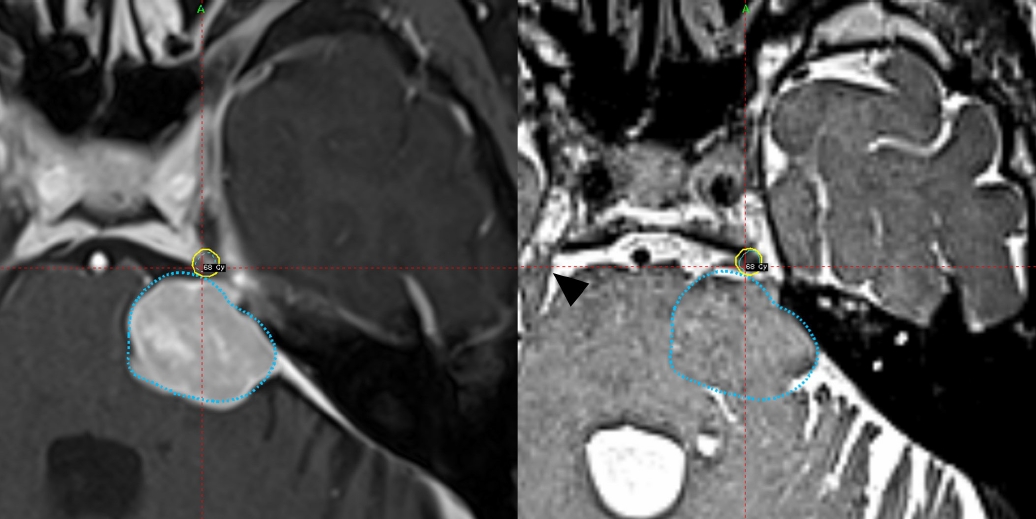
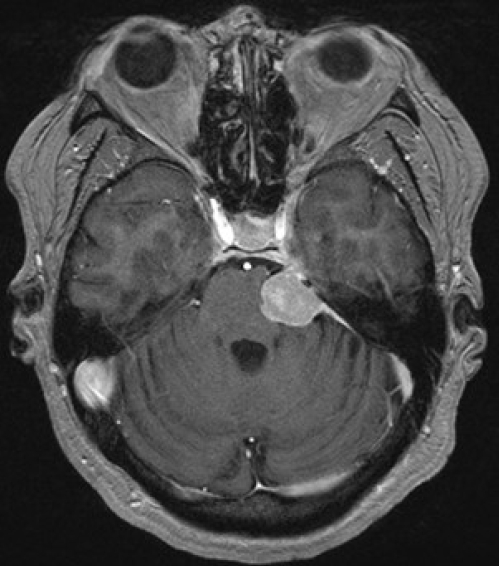
A female 55-year-old patient visited department of neurology. Her chief complaint was left facial pain started 8 months earlier. She experienced stabbing pain in episodic pattern, which was triggered by chewing. The intensity of the pain was as 2-3 on visual analogue scale with three different medications (amitriptyline, gabapentin, carbamazepine). The patient was not treated with topical injection, or any other invasive modalities. A magnetic resonance imaging (MRI) performed and revealed a left CPA meningioma compressing the paraganglion segment of the left trigeminal nerve. GKRS was chosen as the initial treatment because the size of the tumor was within GKRS indication (1.9×1.6×2.2 cm) and the pain was manageable (Barrow Neurological Institute [BNI] pain scale IIIb) (Fig. 1).
The first GKRS was done. A follow-up MRI with Leksell frame for the planning showed no change in tumor size from the 1-month earlier MRI. The radiation target was the tumor, and the dose delivered was 13 Gy (total volume, 3,932 mm2; coverage, 0.97; selectivity, 0.95; isodense line, 3,819 mm2; conformity index, 0.92) (Fig. 2). One month later, however, at the first outpatient visit following GKRS, the patient reported worsened pain. Pregabalin at a dose of 100 mg was added to her prescription. During the second visit, 4 months after GKRS, the patient required additional medication as her pain increased, and the pregabalin dosage was increased to 300 mg.
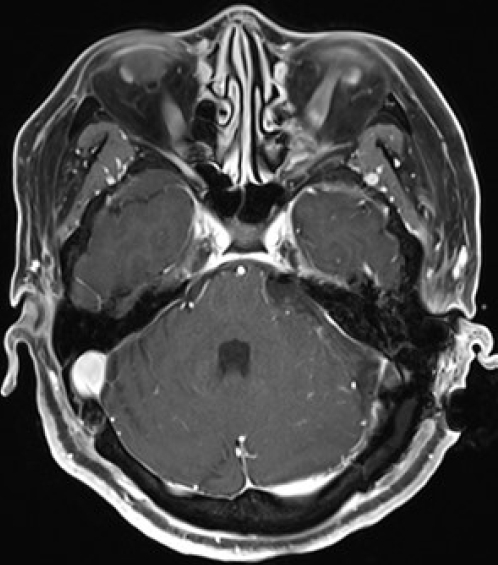
On 6 months after GKRS, the first follow-up MRI revealed a decrease in tumor size (Fig. 3). However, the pain worsened, particularly in the morning (BNI IV). Subsequent follow-up visits did not show any improvement in the aggravated pain, leading to a second MRI 1 year after GKRS to investigate potential reasons for uncontrolled pain, such as edema or tumor growth. However, the tumor showed no increase in size or edema, leading to the decision to perform a second GKRS (Fig. 4).
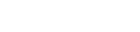
The second GKRS, which targeted the trigeminal nerve, was carried out 15 months after the first GKRS. The dose was 85 Gy in maximum (68 Gy at 80% isodose) (Fig. 3). The second GKRS was expected to liberate the patient from suffering, but the pain only waxed and waned for 7 months, and not relieved. Therefore, the surgical resection of the tumor was decided on May 12th, 2021.
The tumor was surgically resected. Affected trigeminal nerve was compressed with rubber-like mass with moderated adhesion. Also, compressed trigeminal nerve was atrophied and showed indentation (Fig. 5). Postoperative MRI revealed that tumor was successfully removed (Fig. 6). And histopathology reported that the tumor was meningothelial meningioma (World Health Organization grade I). The patient was hospitalized for 7 days after the surgery. Although transient hearing loss occurred on the ipsilateral side, it eventually recovered, and no other complications were reported.
Following tumor resection, the patient still experiences pain, albeit at a reduced intensity (BNI IIIb). Hemifacial paresthesia persists, but overall, the pain scale has improved compared to the initial visit. On her regular following and MRI at out-patient division, there is no sign of any recurrence and the symptoms have relived gradually. At the last visit, she exhibited dysesthesia without pain.
The institutional review board (IRB) of Korea University Guro Hospital approved this retrospective study (IRB No: 2023GR0266), and the need for obtaining informed consent was waived.
DISCUSSION
TN is an oro-facial along trigeminal nerve dermatome. It can manifest as paroxysmal, persistent, or both. The annual diagnosis rate of new TN cases is 4.3 to 27 per 100,000 people. The incidence is higher in women and increases with age [3]. TN can be classified in idiopathic, classic, or secondary. Regardless of the classification, demyelination and axonal dysfunction are known to be the pathophysiology of the TN and it makes the same first choice of therapy, medical treatment [4]. However, when medical treatments fail, secondary treatment options must be pursued based on individual underlying pathology. For classic trigeminal neuralgia (CTN), microvascular decompression may be considered, while surgical removal is often necessary for secondary TN. In addition to these treatments, SRS is a minimally invasive option that can be performed for both CTN and STN.
But SRS has an obvious disadvantage. It takes time for the effects of SRS to manifest, and even more time to determine treatment failure. Time to pain relief following SRS for STN resulting from benign tumors has been reported to range from 4 to 10.5 months and one study reported it may take 49 months from SRS targeted to the tumor to pain relief [1,2]. Indeed, the absence of definitive cut-off value for determining treatment failure with SRS can make it challenging for physicians to transition to the second treatment option.
In this case, the patient presented with TN secondary to the CPA meningioma. As the medical treatment was failed to control the symptoms, the second-line treatment options were necessary. The option that needed to be considered were SRS or surgical resection. Pain relief after SRS of patient in BNI I-IIIb STN patient is known to be 29.8-52.7% and time to pain relief is 4.7-10.5 months [1]. However, as previously discussed, determining treatment failure is challenging, and many patients may need to wait without experiencing improvement. However, for the 8 months following the second GKRS, our patient experienced further worsening of the pain. The BNI pain scale increased from IIIb to IV. The failure of the second GKRS could have been predicted based on the poor response after the first GKRS, which is one of the negative predictors for pain cessation [5].
When the first SRS failed, the subsequent treatment option varied. Secondary SRS to the tumor, additional SRS to the nerve, surgical resection could be considered. SRS on the nerve following SRS on the tumor has been associated with better outcome in patients who did not respond well to the first SRS [6]. However, the patient in this case, she did not respond to two times of GKRS. Thus, the third treatment option is obvious. Surgical resection should be done.
Compared to other treatment modalities, surgical resection has demonstrated most favorable outcomes in pain relief [7]. The development of SRS had led physicians to consider it as the first treatment option, but still open surgery is the most favorable one. It is also obvious that SRS has much more advantages in invasiveness, duration of hospital stays, costs. Upon retrospective review of this case, GKRS remains a viable option as an initial treatment. However, physicians must be aware of different rate of pain relieving of open surgery and SRS. Based on its superior pain relief outcomes, open surgery may be considered as the preferred first treatment option for STN, unless there are absolute or relative contraindications.
CONCLUSION
The volumetric change of a meningioma after SRS is slow, and it may be challenging to anticipate trigeminal pain relief solely from tumor shrinkage. Surgical resection may be considered as the primary option for meningiomas with secondary trigeminal neuralgia or in cases of inadequate pain control following the initial SRS treatment for meningioma. Of course, one should carefully weigh the potential complications of surgical resection when deciding on the primary treatment option.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






